Social media has convinced a generation of women that plastic surgery is like ordering off a menu. You pick a profile, you pick a CC count, and you demand that result.
That approach is inaccurate and, in my private practice, irrelevant.
True aesthetic medicine, the kind we practice in Hinsdale, is about proportion. A 400cc implant on a petite frame doesn't look natural or proportional, it looks obstructive. It practically announces that you had surgery.
My objective is different. I aim for a result that is undetectable to everyone but you and your partner. We're here to restore the anatomical integrity of your body.
1 of 41
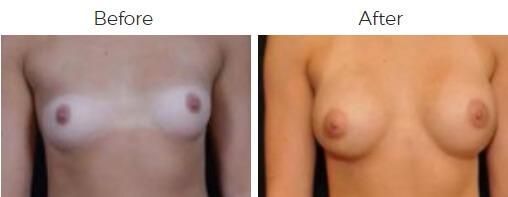
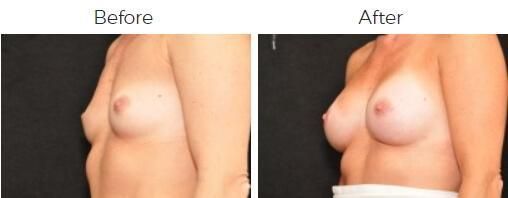
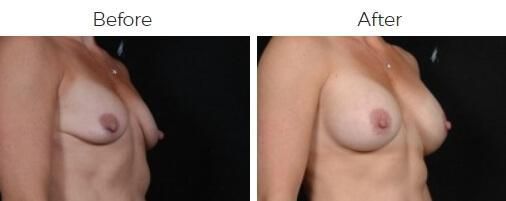
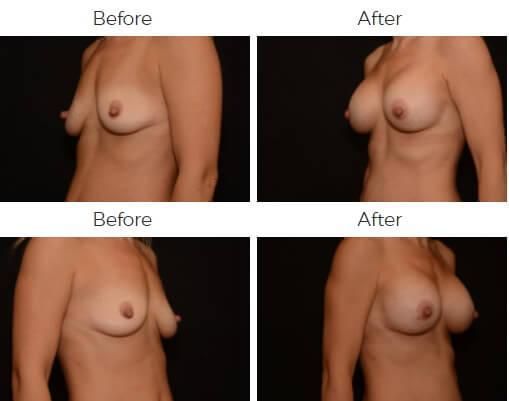
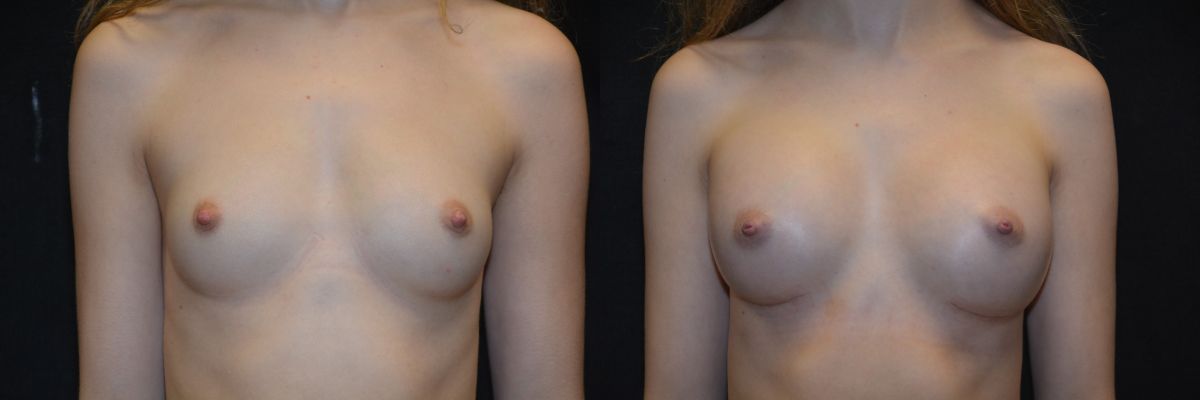
At our office in Hinsdale, IL breast augmentation is a surgical restructuring of the chest wall using silicone or saline implants. We use these devices to increase volume, correct congenital asymmetry, and restore the upper-pole fullness that is inevitably lost after weight fluctuation or breastfeeding. It's a corrective tool designed to re-establish the architectural balance of the silhouette, ensuring the chest proportion aligns seamlessly with the hips and shoulders.

We perform breast augmentation in Hinsdale, IL to make your silhouette coherent. When done correctly, the benefits are structural.

Your rib cage dictates the limit of how big your breasts can be.
I am selective with my patients. The ideal candidate is healthy, non-smoking, and psychologically stable. You understand that implants are medical devices, not magic wands.
If you have a narrow chest wall (base width), we can't force a wide implant into that pocket without causing rippling or edge visibility. If you have significant ptosis (sagging), an implant alone won't fix it—you're a candidate for a lift, not just a breast augmentation. I will inform you of what would be the best course of action for your specific case during your exam.

With breast augmentation Hinsdale patients get a corrective tool for specific anatomical deficits - not just adding volume.
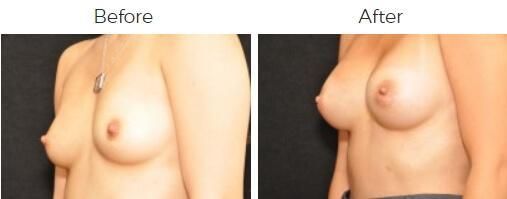
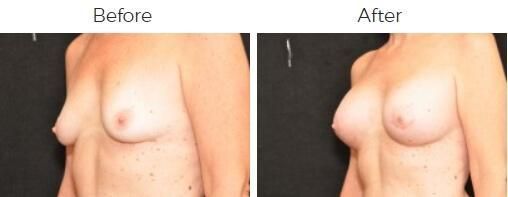
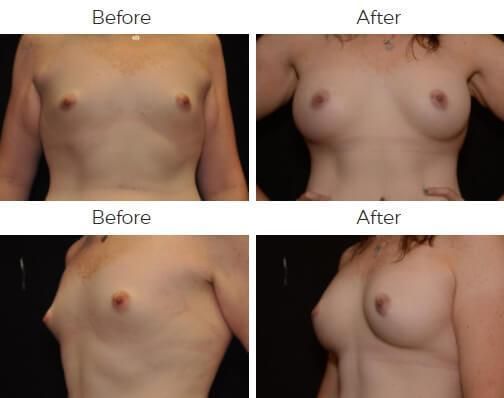
It is rare for a woman to have perfectly symmetrical breasts. Often, one breast is significantly smaller or shaped differently than the other. In these cases, we do not simply use matching implants. We titrate the volume—sometimes using saline for precision or different profile gel implants—to force symmetry where nature failed to provide it.
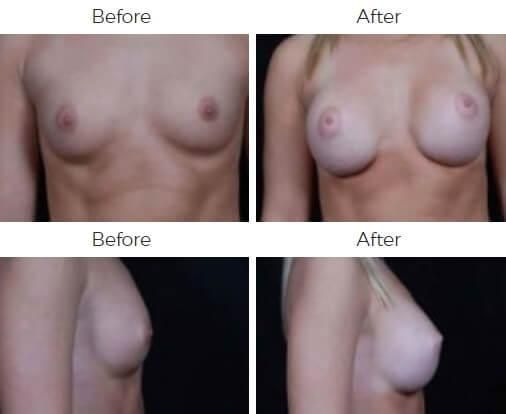
Pregnancy acts like a balloon, inflating and deflating. The skin stretches, but the glandular tissue often atrophies (shrinks) afterward. You are left with a "deflated" look, particularly in the upper pole. An implant acts as a structural filler, returning the breast to its pre-pregnancy tension and shape.
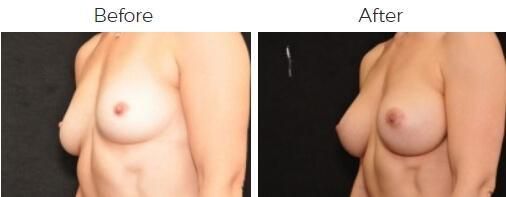
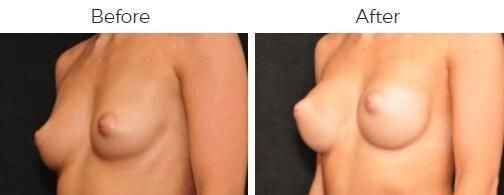
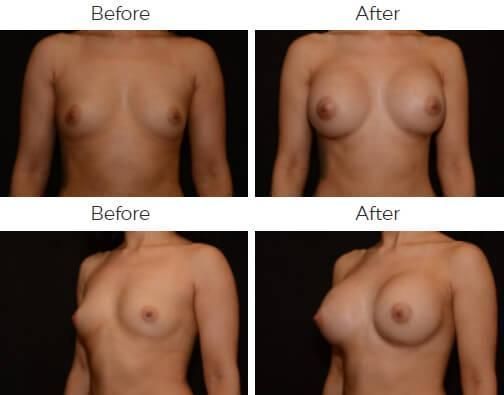
This is a congenital condition where the breast does not develop fully in the lower pole, resulting in a constricted, tube-like shape. Standard augmentation is not enough here. We must release the internal constrictions of the tissue and place the implant specifically to expand the lower breast, unfurling the tissue into a natural teardrop shape.

At Body by Bloch, we do not view breast implants as commodities; we view them as medical devices with specific mechanical properties. We select the material based on the tactile and structural needs of your tissue:
"Profile" is not a style choice; it is a geometrical necessity. The profile determines how far the implant projects forward relative to its width. We select this based on the measurements of your chest wall:
The incision dictates the level of control I have over the surgical pocket. During your consultation, we will select the approach that balances aesthetic discretion with safety:
You can always bring reference photos for what you're looking to have done, but if you walk into a clinic and the plastic surgeon does not measure you, leave.
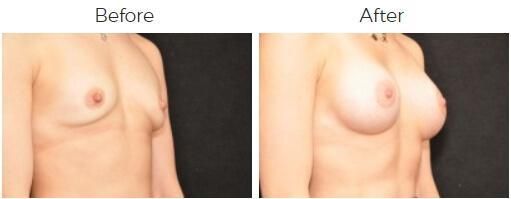
To achieve a sophisticated result, I'll measure the base width of your breast footprint. That measurement is the hard limit. If your breast width is 12cm, and we force a 13.5cm implant into that pocket, the result is a failure.
During the consultation for our Hinsdale breast augmentation, I will hand you the products. You will feel the weight of the cohesive gel. You will understand the trade-offs of texture and projection. We make decisions based on your anatomy, not an Instagram ad.
Some people may claim that putting an implant under the muscle is painful and unnecessary. In reality, it's necessary if you want the edges hidden.
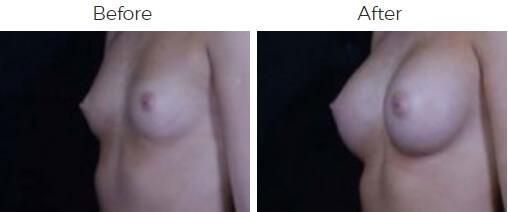
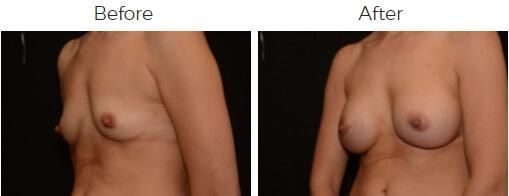
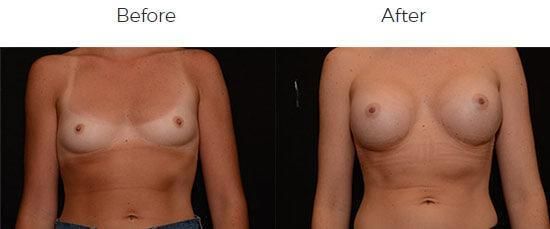
I use a "Dual Plane" technique. I release the pectoralis muscle partially. This allows the top 70% of the implant to sit under the muscle. This provides a soft-tissue blanket that masks the transition from your chest wall—essential for thin patients.
The bottom portion sits behind the breast tissue, allowing the lower pole to expand naturally. This avoids the "ball on a wall" look that characterizes cheap surgery.
If you need to be event-ready within two weeks, you might need to push your surgery off. You will be swollen. Your breasts will be sitting unusually high. Things aren't going to be looking their best until the area calms down a few weeks after breast surgery.
When we place an object under a muscle, the muscle reacts. It tightens. It pushes the implant flat. It's physiology.
Most patients return to desk work in 4 days. You can drive once you cease narcotics. You can handle light life administrative tasks immediately, but you'll still see swelling.
The Rules:
If you compromise the pocket because you wanted to do Pilates, you compromise your results.

Don't judge your result on day one. You will look high and square.
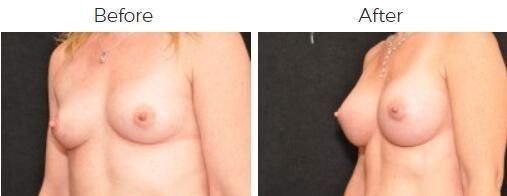
Over the first six weeks, the muscle yields. The implant drops into the pocket. The lower pole rounds out. This is the "Drop and Fluff" phase.
While breast implants are not lifetime devices, many of my patients enjoy their results for 15 to 20 years. If the shell is intact and the aesthetic is good, we leave them alone.
Our pricing reflects the complexity of your case, the caliber of the facility, and the expertise in the room. We don't compete on price because we don't compete on outcome. Services are available for financing if you wish to structure the payment, but the focus here is on the result. We'll give you a full breakdown of the cost during your consultation for breast augmentation in Hinsdale, IL.
You have access to many board-certified plastic surgeons in the Chicago area.
I have been practicing here for over 30 years. I have seen every fad. I have seen every "revolutionary" device that quietly disappeared five years later. I do not experiment on my patients. I use techniques that are proven to last.
When you are in my office, I will highlight what is possible, and I will be blunt about what is not. My staff and team are trained to be equally transparent. We don't sell dreams. We deliver results that are naturally beautiful and long-lasting.
Social media can only tell you what's popular. It can't tell you what's possible for your specific frame.
Move from "browsing" to "planning" as soon as you're ready by contacting my office and securing an appointment. Let's work on enhancing your appearance and bringing balance to your mind and body.
Nerves are often stunned during dissection, but sensation typically returns within 3 to 6 months. Permanent loss is rare.
Yes. By using the inframammary fold incision, we avoid transecting the milk ducts entirely.
Rarely. My dissection is precise enough that bleeding is minimal, negating the need for drains in primary cases.
Yes. Tummy tucks, liposuction, and other surgical treatments can be paired with a breast augmentation, often turning it into a "Mommy Makeover." Many patients even schedule Botox, injectables, or skin treatments during their recovery visits.
No, but you must inform the technician. We use techniques that preserve the integrity of the breast tissue, allowing for effective screening.